
The word Leukemia comes from the Greek leukos which means "white" and aima which means "blood". It is CANCER of the blood or bone marrow (which produces blood cells). A person who has leukemia suffers from an abnormal production of blood cells, generally leukocytes (white blood cells).
The DNA of immature blood cells, mainly white cells, becomes damaged in some way. This abnormality causes the blood cells to grow and divide chaotically. Normal blood cells die after a while and are replaced by new cells which are produced in the bone marrow. The abnormal blood cells do not die so easily, and accumulate, occupying more and more space. As more and more space is occupied by these faulty blood cells there is less and less space for the normal cells - and the sufferer becomes ill. Quite simply, the bad cells crowd out the good cells in the blood.
In order to better understand what goes on we need to have a look at what the bone marrow does.
There are two types of bone marrow: 1. Red marrow, made up mainly of myeloid tissue. 2. Yellow marrow, made up mostly of fat cells. Red marrow can be found in the flat bones, such as the breast bone, skull, vertebrae, shoulder blades, hip bone and ribs. Red marrow can also be found at the ends of long bones, such as the humerus and femur.
White blood cells (lymphocytes), red blood cells and platelets are produced in the red marrow. Red blood cells carry oxygen, white blood cells fight diseases. Platelets are essential for blood clotting. Yellow marrow can be found in the inside of the middle section of long bones.
If a person loses a lot of blood the body can convert yellow marrow to red marrow in order to raise blood cell production.
White blood cells, red blood cells and platelets exist in plasma - Blood plasma is the liquid component of blood, in which the blood cells are suspended.
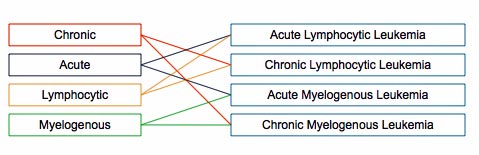
Experts divide leukemia into four large groups, each of which can be Acute, which is a rapidly progressing disease that results in the accumulation of immature, useless cells in the marrow and blood, or Chronic, which progresses more slowly and allows more mature, useful cells to be made. In other words, acute leukemia crowds out the good cells more quickly than chronicleukemia.
Lymphocytic and Myelogenous
Leukemias are also subdivided into the type of affected blood cell. If the cancerous transformation occurs in the type of marrow that makes lymphocytes, the disease is calledlymphocytic leukemia. A lymphocyte is a kind of white blood cell inside your vertebrae immune system. If the cancerous change occurs in the type of marrow cells that go on to produce red blood cells, other types of white cells, and platelets, the disease is called myelogenous leukemia.
To recap, there are two groups of two groups - four main types of leukemia, as you can see in the illustration below:
ACUTE LYMPHOCYTIC LEUKEMIA(ALL)also known as Acute Lymphoblastic Leukemia - This is the most common type of leukemia among young children, although adults can get it as well, especially those over the age of 65. Survival rates of at least five years range from 85% among children and 50% among adults. The following are all subtypes of this leukemia: precursor B-ACUTE LYMPHOBLASTIC LEUKEMIA precursor T acute lymphoblastic leukemia, Burkitt's leukemia, and acute biphenotypic leukemia.
Chronic Lymphocytic Leukemia (CLL) - This is most common among adults over 55, although younger adults can get it as well. CLL hardly ever affects children. The majority of patients with CLL are men, over 60%. 75% of treated CLL patients survive for over five years. Experts say CLL is incurable. A more aggressive form of CLL is B-cell prolymphocytic leukemia.
ACUTE MYELOGENOUS LEUKEMIA(AML) - AML is more common among adults than children, and affects males significantly more often than females. Patients are treated with chemotherapy. 40% of treated patients survive for over 5 years. The following are subtypes of AMS - acute promyelocytic leukemia, acute myeloblastic leukemia, and acute megakaryoblastic leukemia.
Chronic Myelogenous Leukemia (CML) - The vast majority of patients are adults. 90% of treated patients survive for over 5 years. Gleevc (imatinib) is commonly used to treat CML, as well as some other drugs. Chronic monocytic leukemia is a subtype of CML.
As the various types of leukemias affect patients differently, their treatments depend on what type of leukemia they have. The type of treatment will also depend on the patient's age and his state of health.
In order to get the most effective treatment the patient should get treatment at a center where doctors have experience and are well trained in treating leukemia patients. As treatment has improved, the aim of virtually all health care professionals should be complete remission - that the cancer goes away completely for a minimum of five years after treatment.
Treatment for patients with acute leukemias should start as soon as possible - this usually involves induction therapy with chemotherapy, and takes place in a hospital.
When a patient is in remission he will still need consolidation therapy or post induction therapy. This may involve chemotherapy, as well as a bone marrow transplant (allogeneic stem cell transplantation).
If a patient has Chronic Myelogenous Leukemia (CML) his treatment should start as soon as the diagnosis is confirmed. He will be given a drug, probably Gleevec (imatinib mesylate), which blocks the BCR-ABL cancer gene. Gleevec stops the CML from getting worse, but does not cure it. There are other drugs, such as Sprycel (dasatinib) and Tarigna (nilotinb), which also block the BCR-ABL cancer gene. Patients who have not had success with Gleevec are usually given Sprycel and Tarigna. All three drugs are taken orally. A bone marrow transplant is the only current way of curing a patient with CML. The younger the patient is the more likely the transplant will be successful.
Patients with Chronic Lymphocytic Leukemia (CLL) may not receive any treatment for a long time after diagnosis. Those who do will normally be given chemotherapy or monoclonal antibody therapy. Some patients with CLL may benefit from allogeneic stem cell transplantation (bone marrow transplant).
All leukemia patients, regardless of what type they have or had, will need to be checked regularly by their doctors after the cancer has gone (in remission). They will undergo exams and blood tests. The doctors will occasionally test their bone marrow. As time passes and the patient continues to remain free of leukemia the doctor may decide to lengthen the intervals between tests.
The DNA of immature blood cells, mainly white cells, becomes damaged in some way. This abnormality causes the blood cells to grow and divide chaotically. Normal blood cells die after a while and are replaced by new cells which are produced in the bone marrow. The abnormal blood cells do not die so easily, and accumulate, occupying more and more space. As more and more space is occupied by these faulty blood cells there is less and less space for the normal cells - and the sufferer becomes ill. Quite simply, the bad cells crowd out the good cells in the blood.
In order to better understand what goes on we need to have a look at what the bone marrow does.
Function of the bone marrow
The bone marrow is found in the inside of bones. The marrow in the large bones of adults produces blood cells. Approximately 4% of our total bodyweight consists of bone marrow.There are two types of bone marrow: 1. Red marrow, made up mainly of myeloid tissue. 2. Yellow marrow, made up mostly of fat cells. Red marrow can be found in the flat bones, such as the breast bone, skull, vertebrae, shoulder blades, hip bone and ribs. Red marrow can also be found at the ends of long bones, such as the humerus and femur.
White blood cells (lymphocytes), red blood cells and platelets are produced in the red marrow. Red blood cells carry oxygen, white blood cells fight diseases. Platelets are essential for blood clotting. Yellow marrow can be found in the inside of the middle section of long bones.
If a person loses a lot of blood the body can convert yellow marrow to red marrow in order to raise blood cell production.
White blood cells, red blood cells and platelets exist in plasma - Blood plasma is the liquid component of blood, in which the blood cells are suspended.
Types of leukemia
Chronic and AcuteExperts divide leukemia into four large groups, each of which can be Acute, which is a rapidly progressing disease that results in the accumulation of immature, useless cells in the marrow and blood, or Chronic, which progresses more slowly and allows more mature, useful cells to be made. In other words, acute leukemia crowds out the good cells more quickly than chronicleukemia.
Lymphocytic and Myelogenous
Leukemias are also subdivided into the type of affected blood cell. If the cancerous transformation occurs in the type of marrow that makes lymphocytes, the disease is calledlymphocytic leukemia. A lymphocyte is a kind of white blood cell inside your vertebrae immune system. If the cancerous change occurs in the type of marrow cells that go on to produce red blood cells, other types of white cells, and platelets, the disease is called myelogenous leukemia.
To recap, there are two groups of two groups - four main types of leukemia, as you can see in the illustration below:
ACUTE LYMPHOCYTIC LEUKEMIA(ALL)also known as Acute Lymphoblastic Leukemia - This is the most common type of leukemia among young children, although adults can get it as well, especially those over the age of 65. Survival rates of at least five years range from 85% among children and 50% among adults. The following are all subtypes of this leukemia: precursor B-ACUTE LYMPHOBLASTIC LEUKEMIA precursor T acute lymphoblastic leukemia, Burkitt's leukemia, and acute biphenotypic leukemia.
Chronic Lymphocytic Leukemia (CLL) - This is most common among adults over 55, although younger adults can get it as well. CLL hardly ever affects children. The majority of patients with CLL are men, over 60%. 75% of treated CLL patients survive for over five years. Experts say CLL is incurable. A more aggressive form of CLL is B-cell prolymphocytic leukemia.
ACUTE MYELOGENOUS LEUKEMIA(AML) - AML is more common among adults than children, and affects males significantly more often than females. Patients are treated with chemotherapy. 40% of treated patients survive for over 5 years. The following are subtypes of AMS - acute promyelocytic leukemia, acute myeloblastic leukemia, and acute megakaryoblastic leukemia.
Chronic Myelogenous Leukemia (CML) - The vast majority of patients are adults. 90% of treated patients survive for over 5 years. Gleevc (imatinib) is commonly used to treat CML, as well as some other drugs. Chronic monocytic leukemia is a subtype of CML.
Symptoms of leukemia
- Blood clotting is poor - As immature white blood cells crowd out blood platelets, which are crucial for blood clotting, the patient may bruise or bleed easily and heal slowly - he may also develop petechiae (a small red to purple spot on the body, caused by a minor hemorrhage).
- Affected immune system - The patient's white blood cells, which are crucial for fighting off infection, may be suppressed or not working properly. The patient may experience frequent infections, or his immune system may attack other good body cells.
- Anemia - As the shortage of good red blood cells grows the patient may suffer from anemia- this may lead to difficult or labored respiration (dyspnea) and pallor (skin has a pale color caused by illness).
- Other symptoms - Patients may also experience nausea, fever, chills, night sweats, flu-like symptoms, and tiredness. If the liver or spleen becomes enlarged the patient may feel full and will eat less, resulting in weight loss. headache is more common among patients whose cancerous cells have invaded the CNS (central nervous system).
- Precaution - As all these symptoms could be due to other illnesses. A diagnosis of leukemia can only be confirmed after medical tests are carried out.
What causes leukemia?
Experts say that different leukemias have different causes. The following are either known causes, or strongly suspected causes:- Artificial ionizing radiation
- Viruses - HTLV-1 (human T-lymphotropic virus) and HIV (human immunodeficiency virus)
- Benzene and some petrochemicals
- Alkylating chemotherapy agents used in previous cancers
- Maternal fetal transmission (rare)
- Hair dyes
- Genetic predisposition - some studies researching family history and looking at twins have indicated that some people have a higher risk of developing leukemia because of a single gene or multiple genes.
- Down Syndrome - people with Down syndrome have a significantly higher risk of developing leukemia, compared to people who do not have Down syndrome. Experts say that because of this, people with certain chromosomal abnormalities may have a higher risk.
- Electromagnetic energy - studies indicate there is not enough evidence to show that ELF magnetic (not electric) fields that exist currently might cause leukemia. The IARC (International Agency for Research on Cancer) says that studies which indicate there is a risk tend to be biased and unreliable.
Treatments for leukemia
In order to get the most effective treatment the patient should get treatment at a center where doctors have experience and are well trained in treating leukemia patients. As treatment has improved, the aim of virtually all health care professionals should be complete remission - that the cancer goes away completely for a minimum of five years after treatment.
Treatment for patients with acute leukemias should start as soon as possible - this usually involves induction therapy with chemotherapy, and takes place in a hospital.
When a patient is in remission he will still need consolidation therapy or post induction therapy. This may involve chemotherapy, as well as a bone marrow transplant (allogeneic stem cell transplantation).
If a patient has Chronic Myelogenous Leukemia (CML) his treatment should start as soon as the diagnosis is confirmed. He will be given a drug, probably Gleevec (imatinib mesylate), which blocks the BCR-ABL cancer gene. Gleevec stops the CML from getting worse, but does not cure it. There are other drugs, such as Sprycel (dasatinib) and Tarigna (nilotinb), which also block the BCR-ABL cancer gene. Patients who have not had success with Gleevec are usually given Sprycel and Tarigna. All three drugs are taken orally. A bone marrow transplant is the only current way of curing a patient with CML. The younger the patient is the more likely the transplant will be successful.
Patients with Chronic Lymphocytic Leukemia (CLL) may not receive any treatment for a long time after diagnosis. Those who do will normally be given chemotherapy or monoclonal antibody therapy. Some patients with CLL may benefit from allogeneic stem cell transplantation (bone marrow transplant).
All leukemia patients, regardless of what type they have or had, will need to be checked regularly by their doctors after the cancer has gone (in remission). They will undergo exams and blood tests. The doctors will occasionally test their bone marrow. As time passes and the patient continues to remain free of leukemia the doctor may decide to lengthen the intervals between tests.

